
Testosterone Replacement Therapy (TRT) for Women
Testosterone Production in Women
Testosterone is produced in the ovaries, adrenal gland, and through peripheral conversion from circulating androgens. Testosterone levels in women decline significantly with age.
- By age 40, most women have lost about ½ the testosterone they had when they were 20.
- Ovaries continue to make T even after Estrogen production stops
- Testosterone production from adrenal glands declines with aging, but continues post-menopause.
- Women with bilateral salpingo oophorectomy (BSO) have 50% further decline.
References:
Glaser R. York A.E. Dimitrakakis C. Beneficial effects of testosterone therapy in women measured by the validated Menopause Rating Scale (MRS). Maturitas. 2011; 68: 355-361
Glaser, R., Kalantaridou, S., & Dimitrakakis, C. (2013). Testosterone implants in women: pharmacological dosing for a physiologic effect. Maturitas, 74(2), 179–184

The Facts About Testosterone
- Between ages 20 and 40, women can lose 50% of their testosterone production
- Between ages 30-70, men can lose 1-3% of total testosterone production per year
- As humans age, a significant change occurs in the balance of albumin and SHBG. Albumin is a protein found in the body that binds to and transports testosterone. Sex-Hormone Binding Globulin (SHBG) is a protein that binds to, transports and inhibits the function of testosterone. SHBG controls the amount of testosterone an individual’s body tissues can use.
References:
Tetsuo Hayashi & Takumi Yamada (2008) Association of bioavailable estradiol levels and testosterone levels with serum albumin levels in elderly men, The Aging Male, 11:2, 63-70, DOI: 10.1080/13685530701779234

Testosterone Method of Delivery (and Why it Matters)
ORAL:
- Requires daily administration.
- First-pass effect (pharmacological phenomenon in which a medication undergoes metabolism at a specific location in the body and decreases the active drug’s concentration upon reaching systemic circulation or its site of action)
- May cause GI upset or nausea.
- Not as effective as other methods.
- Methyltestosterone can sometimes cause hepatotoxicity, for instance elevated liver enzymes, cholestatic jaundice, peliosis hepatis, hepatomas, and hepatocellular carcinoma, with extended use.
- With buccal/sublingual forms, must be dosed 3x per day.
TRANSDERMAL:
- Requires daily or twice daily administration.
- Avoids first-pass metabolism by the liver.
- Can cause skin irritation
- Some individuals are unable to properly absorb.
- Blood levels will vary.
- Possible transfer to others through skin-to-skin contact.
INJECTABLE:
- Weekly or biweekly administration.
- Inconsistent, fluctuating levels, creating a “roller coaster” effect.
- Hormone level rapidly increases.
- Injection causes some pain.
- Some individuals may have allergic reaction to carrier oils
PELLET:
- Administered every 3 or 4 months based on gender.
- Provide steady, stable hormone levels over time.
- Minimal time and discomfort associated with insertion.
- Extremely low level of pellet extrusion.
- Most patients return to normal activities minutes after treatment.
- Dose adjustments are made by assessing response and follow up blood work.
References:
Čeponis, J., Yadav, P., Swerdloff, R.S., Wang, C. (2017). Testosterone Therapy: Transdermal Androgens. In: Hohl, A. (eds) Testosterone. Springer, Cham. https://doi.org/10.1007/978-3-319-46086-4_11
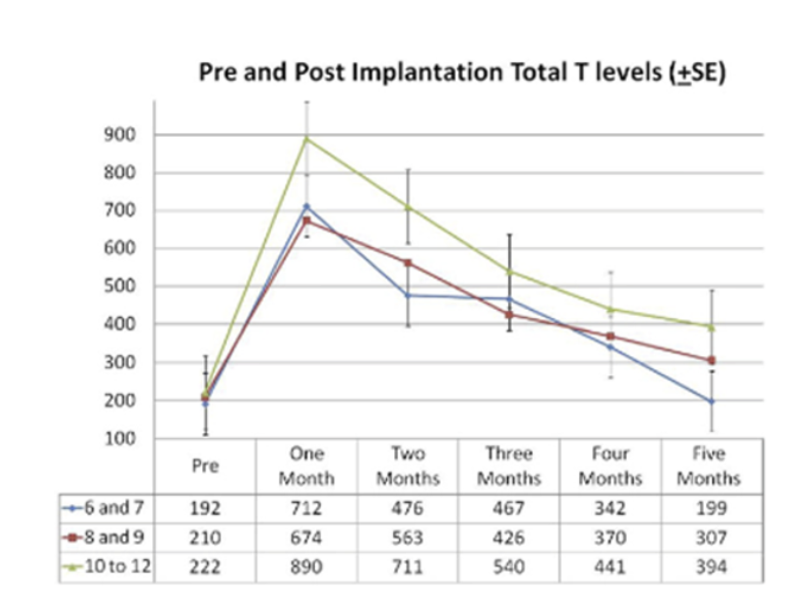
Testosterone Pellets
- Multiple and customized dosing options.
- Consistent, steady levels.
- Predictable absorption.
- Pellets kick in at about a week.
- Patient stops other forms of Testosterone at one week.
- Rise and peak around weeks 4-6.
- Reduced risk of platelet aggregation.
- Convenient option with fewer office visits for maximized patient satisfaction and compliance.
- 1-4 times per year for women.
- 1-3 times per year for men.
References:
1497 A MULTI-INSTITUTIONAL OBSERVATIONAL STUDY ON TESTOSTERONE LEVELS AFTER TESTOSTERONE PELLET (TESTOPEL™) INSERTION Andrew McCullough, Mohit Khera, Wayne Hellstron, Abraham Morgentaler, Larry Levine and Irwin Goldstein
Testosterone and Women: International Expert Consensus Resolutions
- Testosterone is not a male-exclusive hormone. It is the most abundant gonadal hormone throughout a woman’s life.
- Serum testosterone levels do not correlate with symptoms of testosterone deficiency in women. Optimal ranges of serum testosterone levels in women have not been established.
- Female testosterone insufficiency is a clinical syndrome that may occur during any decade of adult life.
- Testosterone therapy may be breast protective.
- Testosterone insufficiency in women negatively affects sexuality, general health and quality of life. Testosterone supplementation may positively influence sexuality, general health and quality of life.
- Testosterone insufficiency may be associated with an increased risk of cardiovascular disease in women.
- Testosterone optimization may be brain protective and may enhance cognitive function.
- Testosterone optimization may be a key component for improved bone health.
- Testosterone therapy in women has no adverse effects on lipids and/or cardiovascular risk.
- Studies of testosterone supplementation show benefits exceed the risk and consistent purity and potency can be achieved.
References:
Gary Donovitz, MD (Chairman), Erika Schwartz, MD, Charles Miller, MD Mickey Barber, MD, Florence Comite, MD, Ken Janson, MD, Jeffrey Leake, MD, Edwin Lee, MD, Jeffry Life, MD, Luis Martinez, MD, Douglas Woodford, MD “Testosterone Insufficiency and Treatment in Women: International Expert Consensus Resolutions”
Signs and Symptoms of Testosterone Deficiency
Common symptoms of testosterone deficiency include the following:
- Insomnia
- Depression
- Headaches
- Worsening of quality of life (mood, affect, energy)
- Vaginal vasocongestion
- Reduced sex drive and enjoyment
- Reduction of pubic hair, bone mass and muscle mass
Benefits of TRT in Women
Benefits often experienced by women who receive Testosterone Replacement Therapy include the following:
- Better sleep
- Reduced “brain fog”
- Enhanced cognitive function
- Increased energy and sense of well being
- Fight effects of osteoporosis
- Stronger bones and skeletal growth
- Lower cholesterol
- Heart protection
- Enhanced libido and sexual function
References:
Clarke BL, Khosla S. Androgens and bone. Steroids. 2009 Mar;74(3):296-305. doi: 10.1016/j.steroids.2008.10.003. Epub 2008 Oct 17. PMID: 18992761; PMCID: PMC2679948.
Deborah R Cameron, Glenn D Braunstein, Androgen replacement therapy in women, Fertility and Sterility, Volume 82, Issue 2, 2004, Pages 273-289, ISSN 0015-0282
The Effect of Testosterone Pellets on Bones
- Testosterone builds and maintains bones.
- Effective for prevention and treatment of osteoporosis.
- In postmenopausal women, treatment with combined estradiol and testosterone implants is more effective than estradiol implants alone.
References:
Zhang H, Ma K, Li RM, Li JN, Gao SF, Ma LN. Association between testosterone levels and bone mineral density in females aged 40-60 years from NHANES 2011-2016. Sci Rep. 2022;12(1):16426. Published 2022 Sep 30. doi:10.1038/s41598-022-21008-7
Davis SR, McCloud P, Strauss BJ, Burger H. Testosterone enhances estradiol’s effects on postmenopausal bone density and sexuality. Maturitas. 1995;21(3):227-236. doi:10.1016/0378-5122(94)00898-h
EMBRACE YOUR BEST SELF
From hormone optimization to cartilage regeneration, we create personalized treatment plans based on thorough testing and monitoring.
We treat our patients for their unique needs and symptoms, rather than simply viewing lab results. We go beyond the numbers to alleviate our patient’s symptoms and get them back to living the lives they want to live.



